


Universal Neonatal Foot Orthotics (UNFO): A Novel Method to correct forefoot adduction, Preliminary report
Avi Panski, Naum Simanovski, Vladimir Goldman, Ron Lamdan Pediatric Orthopedics Unit,
Hadassah medical center, Jerusalem


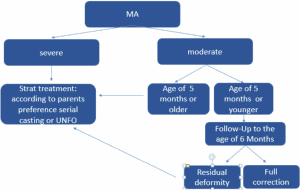
Metatrasus Adductus (MA), what do we know?
The most common foot deformity in newborns: 1-2/1000 births
- severe
- Not correctable past neutral
- Heel bisector at 4th toe or beyond
- Deep medial skin crease
- moderate
- Correctable to neutral
- Heel bisector medial to 4 th toe
- Mild or no skin crease
- Natural History
- Most cases will resolve spontaneously
- 11–14% persistent and require treatment
Treatment of Metatasus Adductus
- Serial casting (best results up to 8-9 month old babies) Occasionally followed by an orthosis
- Time consuming
- messy
- Interferes with bathing & hygiene
- Slippage of the cast
- Pressure sores
- Treatment options in unresolved
Metatarsus adductus among older children
- Ignore
- There is no functional impairment
- Surgery
- Stumbling
- Esthetics
- Footwear
- Social
Materials and methods
- Retrospective study of our first 15 consecutive patients treated with UNFO (June 2014 – November 2015)
- Follow up of 2 months minimum after cessation of treatment
- Treatment protocol:
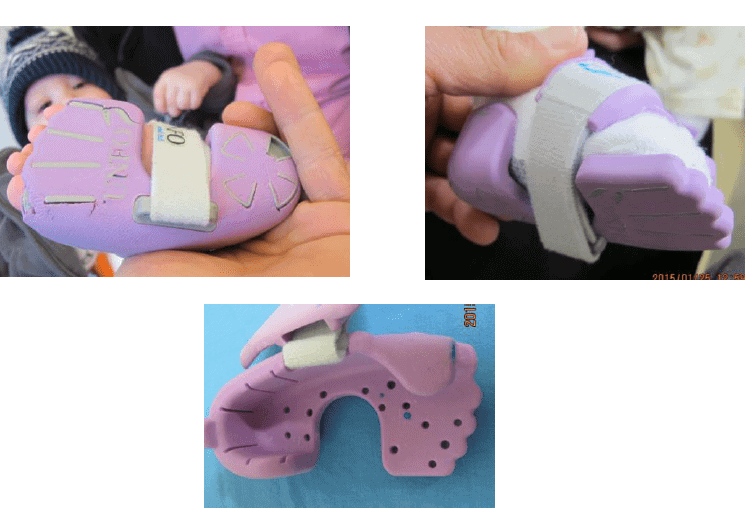
What is UNFO
Universal Foot Orthotics
2 sizes
3 point pressure
Heel held firmly
Point of pressure against the 1st metatarsal head
Strap for increasing pressure gradually over base of 5th metatarsus
UNFO treatment protocol
UNFO was first applied for 23 hours a day
Weaning gradually when full correction was achieved
- 3-4 weeks 18 hours
- 3-4 weeks 12 hours night time
- Stop UNFO
- (if the parents wish, continue night time bracing as long as it fits)
- Follow-up 3 week
- Follow-up when walking
- Follow-up at the age of 1.5 and 2 years
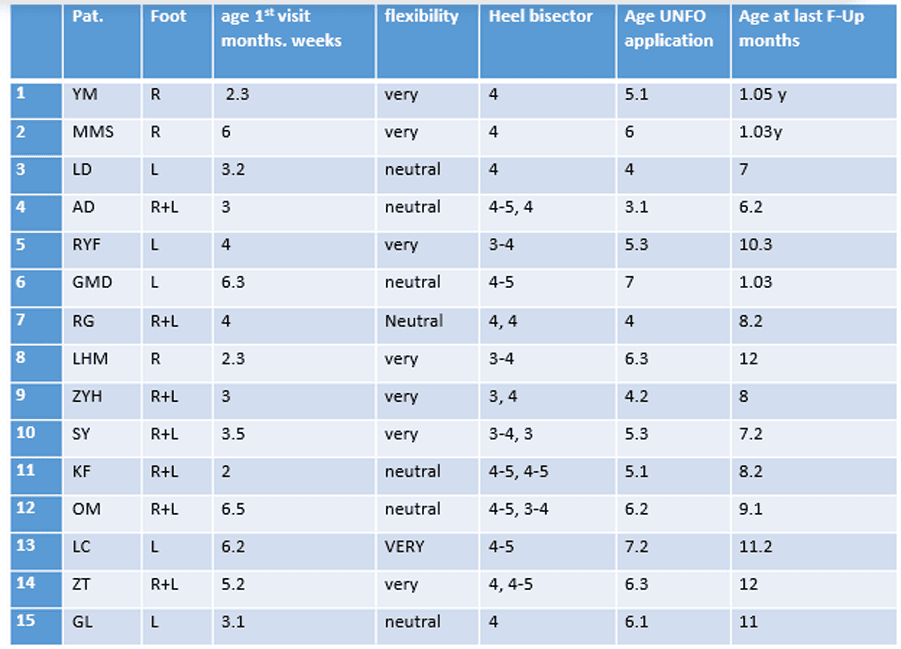
Patients details
Results
- 15 patients, 22 feet (5 Lt 3 Rt 7 bilateral) followed until end of treatment
- 7 Patients severe Metatarsus adductus (11 feet)
- 8 Patients moderate Metatarsus adductus (11 feet)
- Age at beginning of treatment 3.1-7.2 months (average 5 months +2 weeks)
- Time to full correction: following visit (4 days-3 weeks)
- Final outcome – resolution of Metatarsus adductus in all cases
- Side effects – minor
- Superficial wounds 1
- Redness of the skin 4
- Slippage of UNFO 2
- Device wear 1
- Excessive sweating 1
Discussion
About 11–14% of Metatarsus adductus do not resolve spontaneously
- The optimal age for treatment of Metatarsus adductus is up to the age of 9 months
- Treatment options include serial casting or usage of adjustable orthosis
- We present our experience with treatment of Metatarsus adductus among young babies using a new orthosis – UNFO – which fits tightly to the babies foot and by the three-point fixation principle corrects the deformity
- The amount of pressure over the apex of the deformity is controlled by an adjustable velccro strap easy to apply and manipulate by the baby’s caregivers
- This method is better tolerated by the infant and caregivers and is less time and effort consuming then serial casting
- In comparison to the Bebax orthosis UNFO is easily applied and manipulated by one caregiver
- In comparison to the Wheaton brace the advantage of UNFO is leaving the ankle joint and leg out of the brace
- Treatment was begun as soon as the baby was diagnosed as having severe Metatarsus adductus or only if spontaneous resolution has not occurred up to the age of 6 months
- Correction was achieved within 3 weeks with only few minor side effects
Conclusion
- Metatarsus adductus in infants should not be ignored
- Severe deformities or deformities which have not improved spontaneously up to the age of 6 months should be treated
- Treatment with UNFO is a safe and effective method to correct metatarsus adductus deformity in infants up to the age of 9 months
- There were only minor side effects as redness of the skin or superficial wounds which healed after a day or two without the orthosis
- The authors declare of no conflict of interest